
Home Data Center Data Reports Suicide Care in Kentucky Hospitals
When someone dies by suicide, like any cause of death, the loss is felt by many. The ripples of loss spread from close family and friends to community members, acquaintances, and even people the deceased did not know. All of those exposed to the loss may experience different levels of grief and trauma. According to the Centers for Disease Control and Prevention (CDC), an estimated 13.2 million adults seriously thought about suicide, 1.6 million attempted suicide, and there were 49,476 deaths by suicide in 2022, making it the ninth leading cause of death in the United States.1
Suicide is a major, preventable health concern in the United States. While suicide is preventable, it does require intervention. Emergency departments (EDs) are important sites for identifying at-risk individuals, providing timely support and intervention, and facilitating entry into more intensive treatment. All Kentucky hospitals screen patients for suicidal ideation. This practice started in 2023, and and in the past nine months of 2024, hospitals successfully screened ninety-three percent of patients in the emergency department.
This report provides an overview of suicide-related visits (encounters) in Kentucky hospitals and EDs, recent changes, and patient demographics.
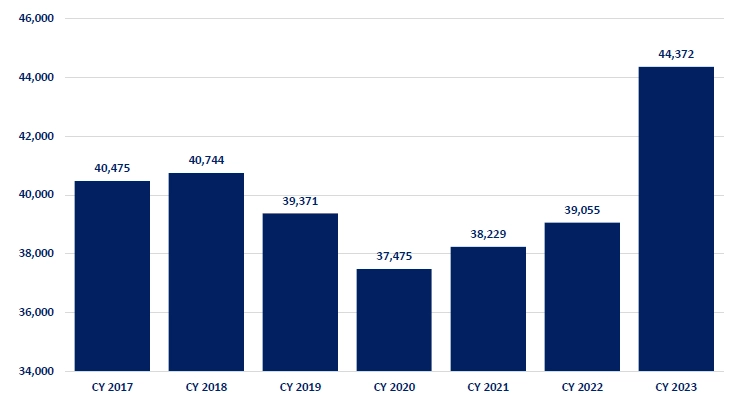
Administrative claims data from Kentucky hospitals shows the changes for suicide-related visits from calendar year (CY) 2017 through CY 2023. The vast majority are diagnoses of suicidal ideation, which were in decline and reached their lowest levels in CY 2020 (37,475) during the COVID-19 pandemic and the associated shutdown of elective procedures (Figure 1a). Diagnoses of suicidal ideation have increased every year since and reached an unprecedented high of 44,372 diagnoses in CY 2023. The especially large increase in diagnoses in CY 2023 is likely due to the adoption of “universal screening” in hospitals.
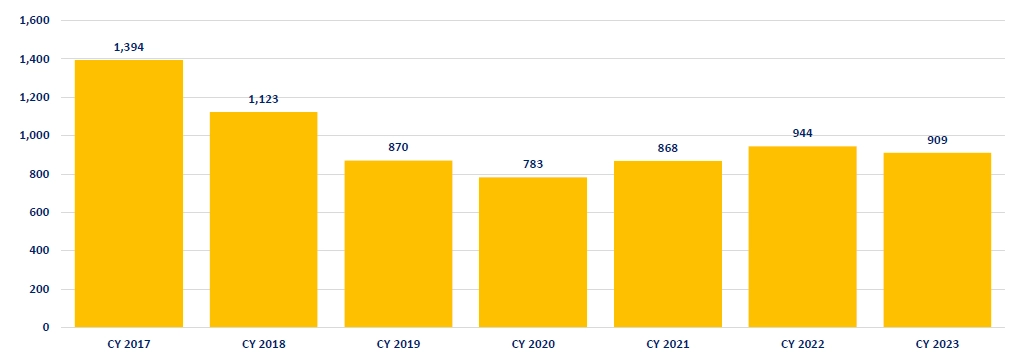
The trend for suicide attempts is similar, with a steady decline until CY 2020, followed by a more modest increase and a recent plateau (Figure 1b). A welcome decrease from a high of 1,394 diagnosed suicide attempts in CY 2017 to 909 in CY 2023, a decrease of 35 percent.
Figure 1 (a). Discharge Diagnosis: Suicidal Ideations, CY 2017 ‐2023
Data Source: KHA InfoSuite
Figure 1 (b). Discharge Diagnosis: Suicide Attempts, CY 2017 ‐2023
Data Source: KHA InfoSuite
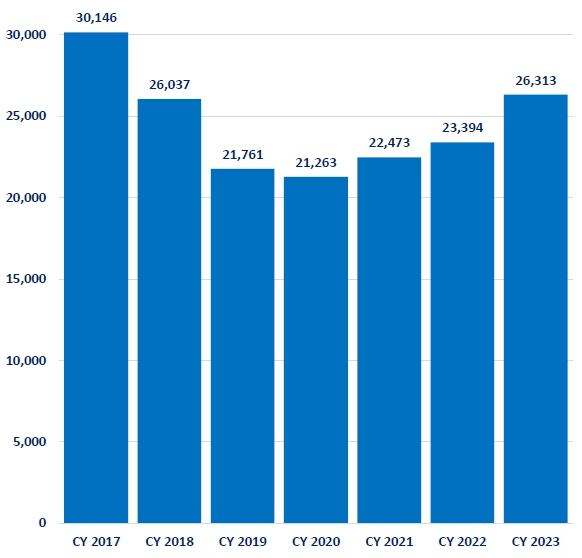
The state-wide prevalence of suicide-related visits in Kentucky hospitals includes all inpatient and outpatient settings. However, most suicide-related visits occur in the ED, although the number has varied over the last few years. Figure 2 shows the number of suicide-related visits in the ED from CY 2017 to 2023. In CY 2017, seventy-two (72) percent of all suicide-related visits (30,146) occurred in the emergency department. Over the next three years, including during the emergence of COVID-19 in CY 2020, the number of suicide-related visits to the ED declined. In CY 2020, the number of suicide-related visits to the ED was at its lowest at 21,263 but has risen every year since and culminated at 26,313 in CY 2023. The aforementioned implementation of screening patients for suicidal ideation will facilitate access to treatment and affect the number of suicide-related visits to the ED.
Figure 2. Suicidal Ideation & Attempts in Emergency Departments, CY 2017 ‐2023
Data Source: KHA InfoSuite
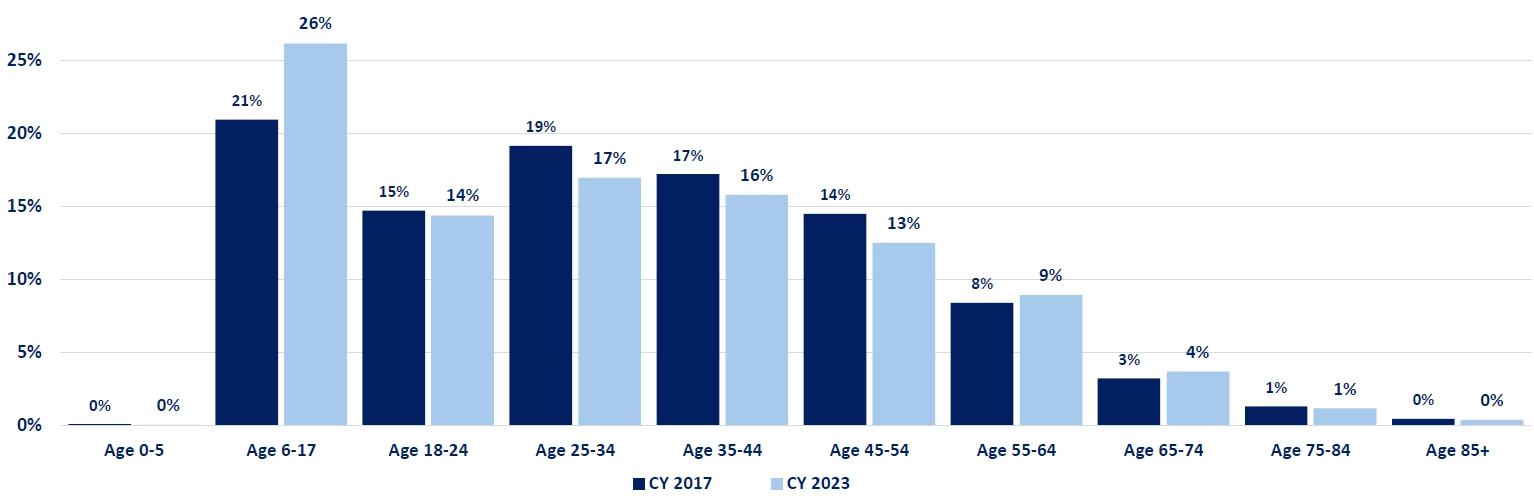
Suicide-related diagnoses are more common among adolescents (ages 16 – 17) and young adults (ages 18-24). Together, these two age groups account for 41 percent of all suicide-related diagnoses in Kentucky hospitals in CY 2023. Figure 3 shows a shift toward adolescents, while older adults age 75 and older make up approximately the same share of suicide-related diagnoses. The share of suicide-related visits decreased between ages 18-54 and shifted towards adolescents.
Figure 3. Suicide‐Related Visits by Age, CY 2017 compared to CY 2023
Data Source: KHA InfoSuite
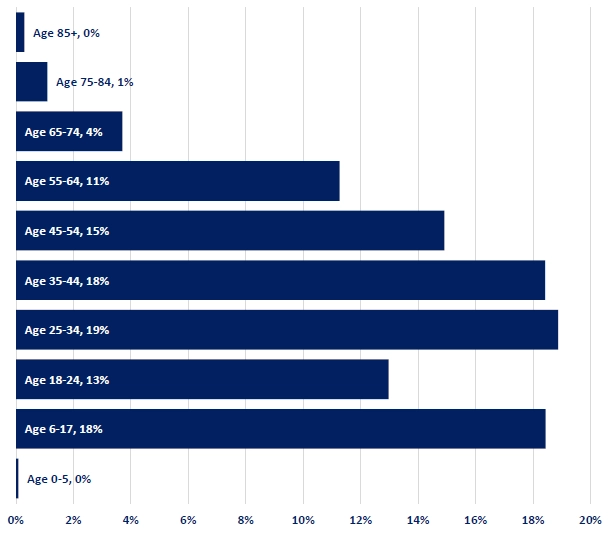
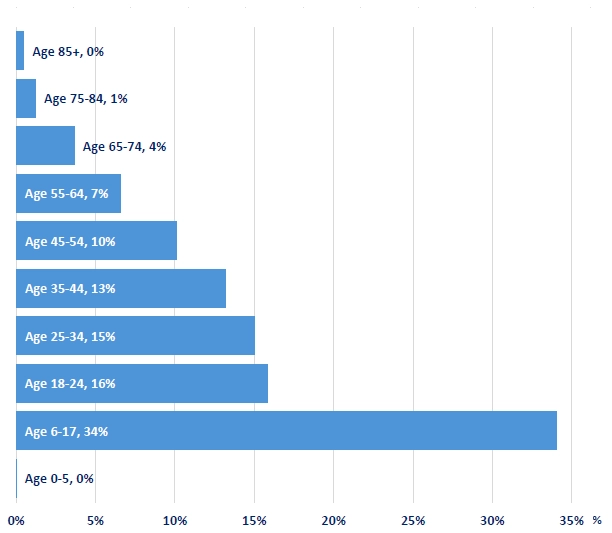
However, there are differences between genders (Figure 4). Almost 50 percent of suicide-related visits for women are among adolescents and young adults, and decline for every age cohort thereafter. While men also have a high rate in adolescence, about 18 percent of all suicide-related visits, ages 25 to 54 account for 52 percent of all cases. In contrast, young men ages 18 to 24 have relatively lower rates, 13 percent, compared to adolescents and older males. In both cases, for men and women, the share of suicide-related visits to the ED for adults aged 75 and older is one percent or less. However, it is still a substantial number of visits, 376 for women and 315 for men, in CY 2023.
Figure 4 (a). Suicide‐Related Visits by Age, Male, CY 2023
Data Source: KHA InfoSuite
Figure 4 (b). Suicide‐Related Visits by Age, Female, CY 2023
Data Source: KHA InfoSuite
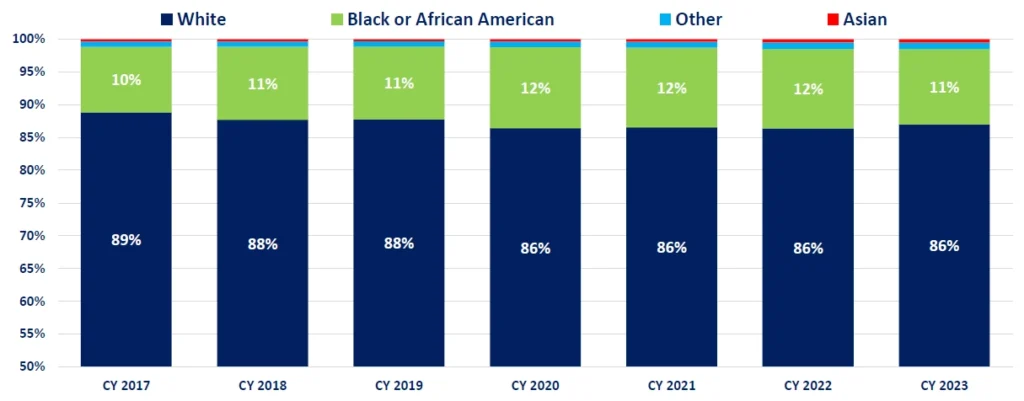
The Kentucky State Data Center (KSDC) at the University of Louisville publishes the official Census data for Kentucky and its estimate shows a population that is 83.2 percent white, 8.4 percent black or African American, 1.7 percent Asian, and 2.4 percent other. Suicide-related visits are similarly distributed in Kentucky (Figure 4b), although somewhat higher for both white (86 percent, CY2023) and black or African American (11 percent, CY2023) and relatively low for Asian and other races (below 1 percent), and largely unchanged for several years.
Figure 5. Suicide-Related Visits by Race, CY 2017-2023
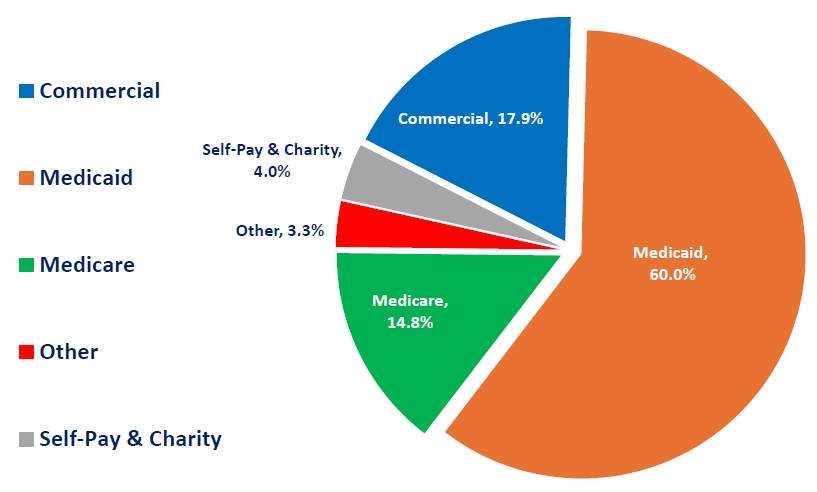
Figure 6 shows that Medicaid pays for the majority of suicide-related visits in Kentucky, 60 percent, nearly two-thirds, compared to a much smaller share in Medicare (15 percent) and commercial insurance (18 percent). The remaining cases are self-pay, third party liability (“Other”), and hospital charity care.
Figure 6. Payer Distribution for Emergency Department Suicide‐Related Visits in CY 2023
Data Source: KHA InfoSuite
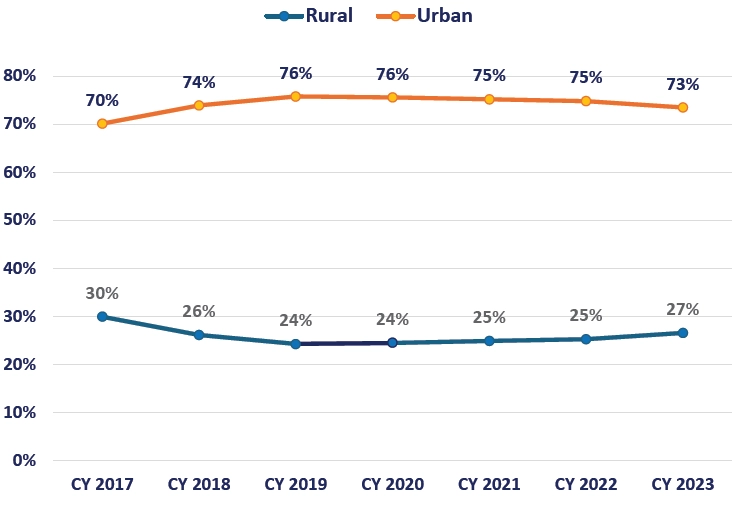
Most suicide-related visits occur in urban hospitals (Figure 7). Even though the exact number of visits fluctuates, urban hospitals provide care to approximately 70 to 76 percent of these patient encounters. Urban hospitals typically report 28,000 to 33,000 suicide-related patient encounters every year, whereas rural hospitals average between 9,000 and 12,000 suicide-related visits per year.
Figure 7. Suicide‐Related Visits: Rural and Urban Hospitals,
CY 2017 ‐2023
Data Source: KHA InfoSuite
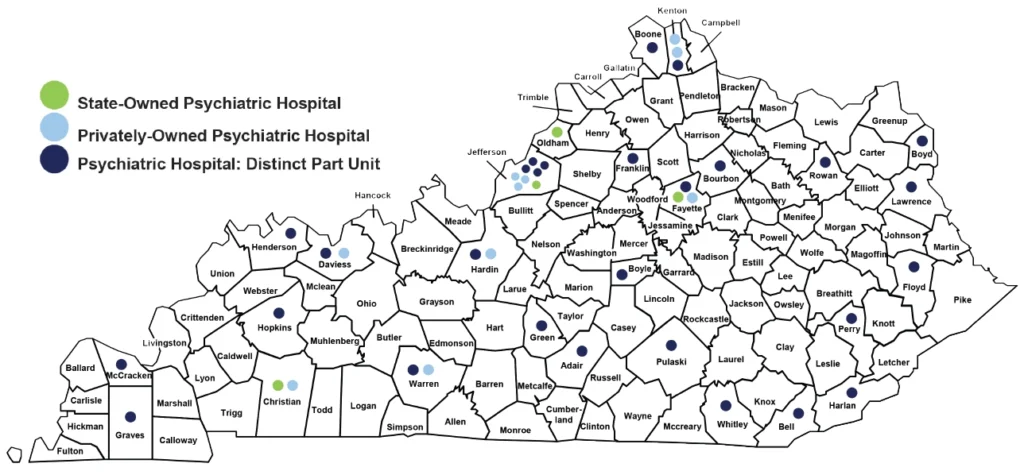
Kentucky hospitals operate different types of facilities, including acute care hospitals, critical access hospitals, psychiatric hospitals, and other specialty hospitals, such as long-term care, pediatric, and rehabilitation hospitals. Most suicide-related diagnoses come from acute care and psychiatric facilities. In CY 2017, nearly 74 percent of suicide-related visits occurred in acute care hospitals, but that has changed, and approximately 35 percent are now reported by psychiatric hospitals, whereas 60 percent of visits are still in acute care hospitals. The following map shows the locations of all psychiatric hospitals in Kentucky.2
Data Source: KHA’s Kentucky Hospital Statistics
Kentuckians in crisis can now connect with suicide prevention, mental health, and substance use counselors using a nationwide, easier-to-dial phone number – 988. Phone service providers will now direct 988 calls to the existing national lifeline with its 13 Kentucky call centers. And connection to additional crisis services will be provided if necessary.
For more information about the KHA Data Center, please contact:
Maik Schutze
Director, Health Information and Analytics
Kentucky Hospital Association
mschutze@kyha.com
1 CDC. https://www.cdc.gov/suicide/facts/index.html
2 The Kentucky Hospitals Association (KHA) also publishes a map of all hospitals with contract information on its website: https://www.kyha.com/about-kha/hospitals/map/